

The referral-to-treatment (RTT) waiting list (probably) got smaller, with the largest October fall since 2008, and waiting times (probably) reduced, especially for those patients waiting for a diagnosis and decision to admit. This is good news at last.
Analysis produced for Health Service Journal by Dr Rob Findlay, Director of Strategic Solutions at Insource Ltd and founder of Gooroo Ltd
But why ‘probably’? Last year NHS England issued a new edition of guidance stating “when a patient declines 2 reasonable offers for earlier treatment dates at an alternative provider – the hospital may decide to commence a period of active monitoring” which removes them from the published waiting list and makes the figures look better even though the number of patients waiting has not really changed. I have argued that this is unlawful, reduces patient choice, and makes the waiting list data less reliable – hence the ‘probably’.
NHS England could, if they chose, publish statistics from the national Waiting List Minimum Data Set (WLMDS) to show how much of the apparent improvement is due to this counting change, but they currently choose not to. In contrast, they do publish WLMDS data when it suits them, to show how much smaller the waiting list would appear if you counted unique patients instead of patient pathways (the NHS’s to-do list being better represented by the latter).
All of that said, an apparent improvement is better than an apparent deterioration. The shorter wait for diagnosis and decision is especially welcome. So let us hope that most of the improvement is genuine and that it continues.
In the following discussion, all figures come from NHS England. You can look up your trust and its prospects for achieving the current waiting time targets here.
The numbers
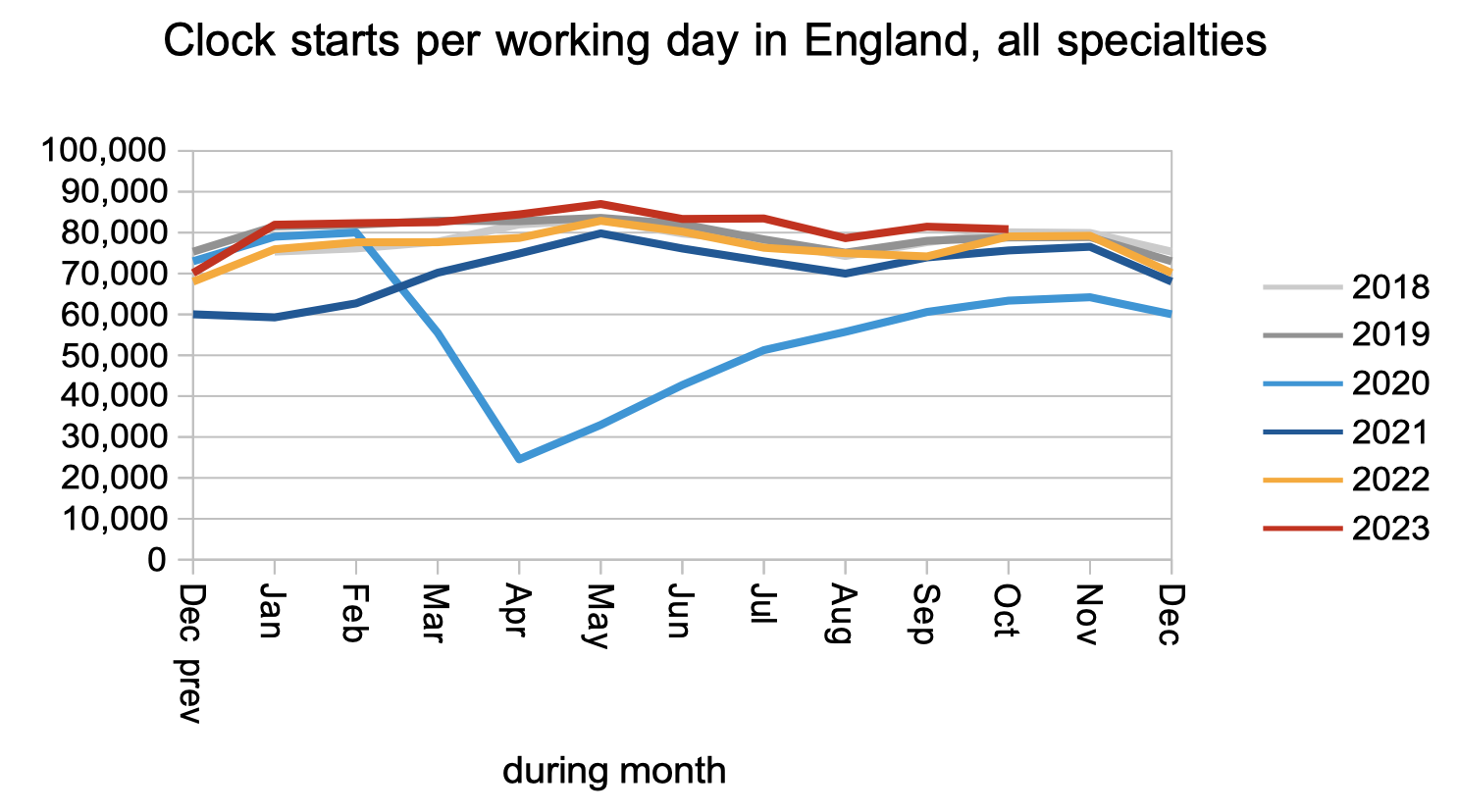
Patients joined the waiting list and started new waiting time ‘clocks’ at slightly higher than pre-pandemic rates, continuing the recent trend.
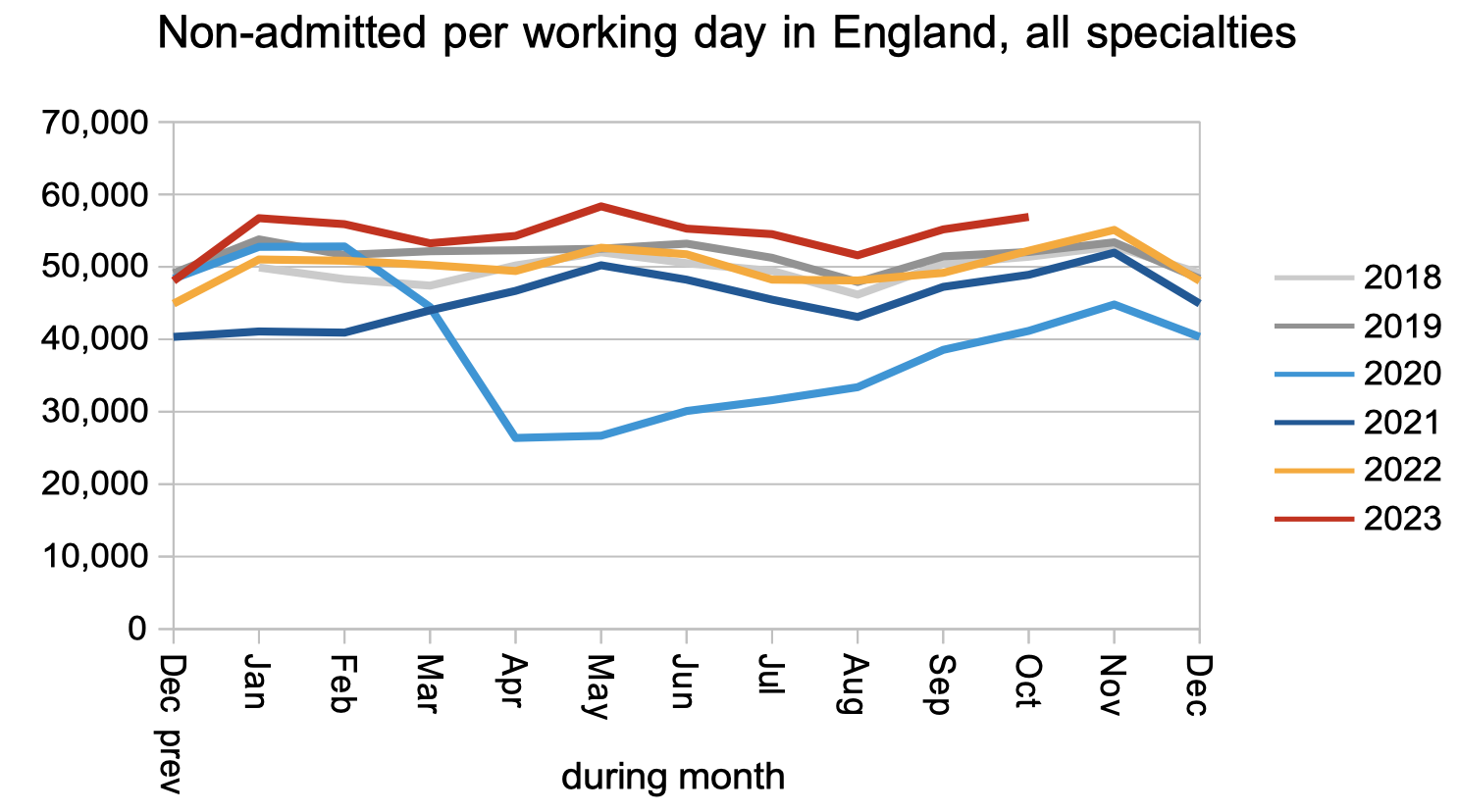
Patients left the waiting list after an outpatient appointment, or were removed administratively, at higher than pre-pandemic rates, again continuing the recent trend. We do not know how much of this is due to the new ‘unlawful’ guidance.
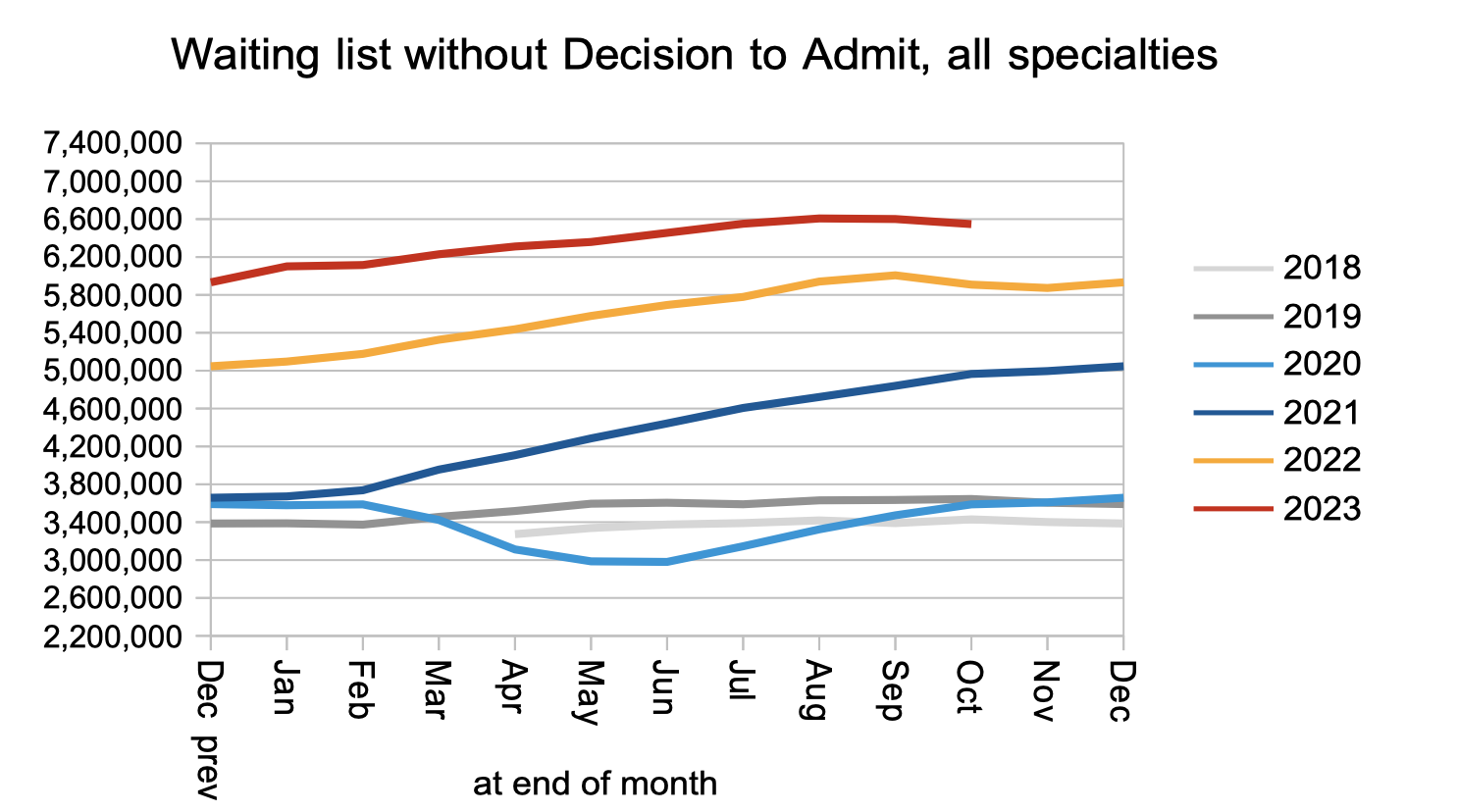
The consequence of those clock starts and clock stops, together with the (unknown) numbers who continued their wait following a Decision to Admit (DTA), was that the number waiting without a DTA fell slightly in October.
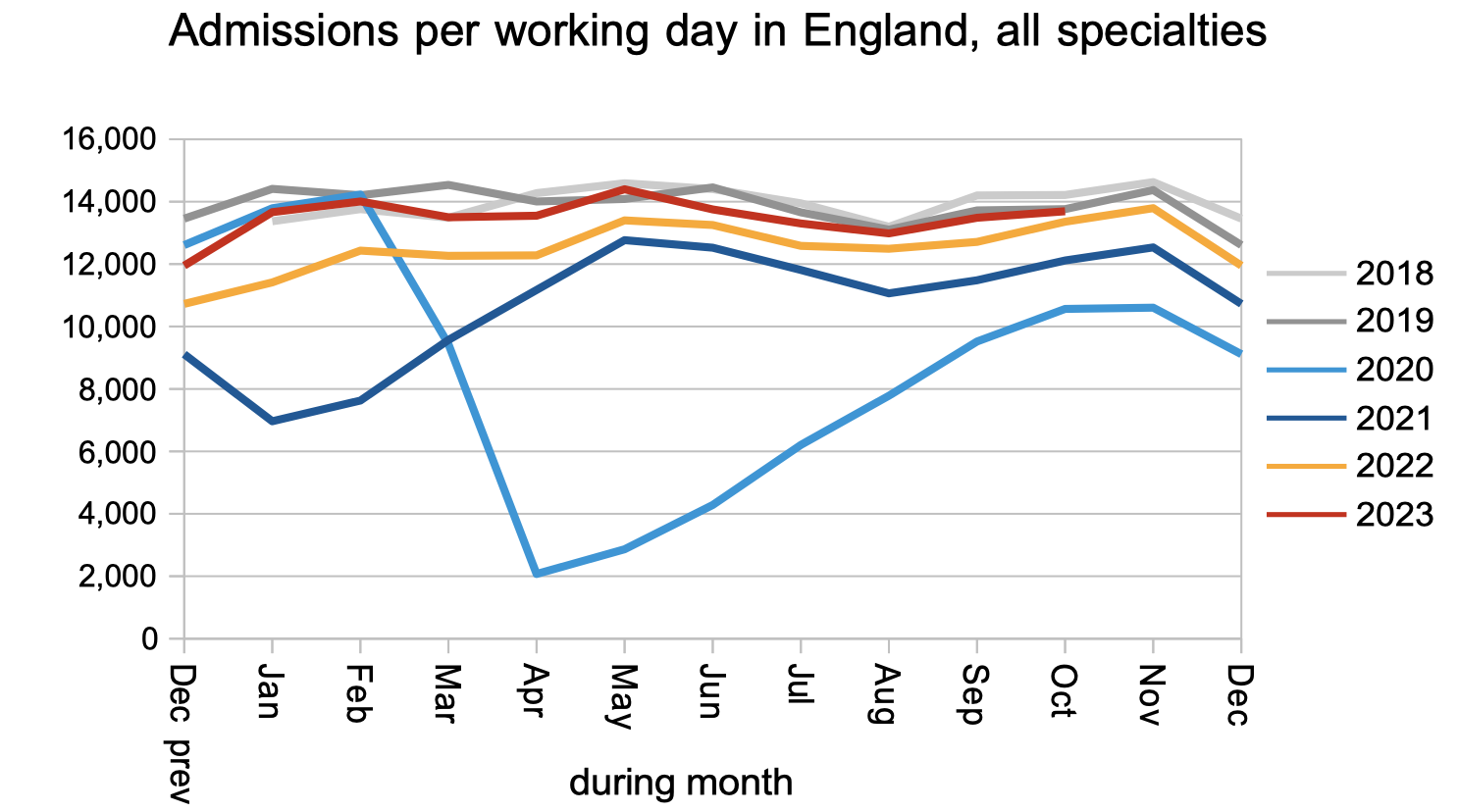
Turning now to those patients who have a Decision to Admit, the number who were actually admitted for treatment remained at pre-pandemic levels.
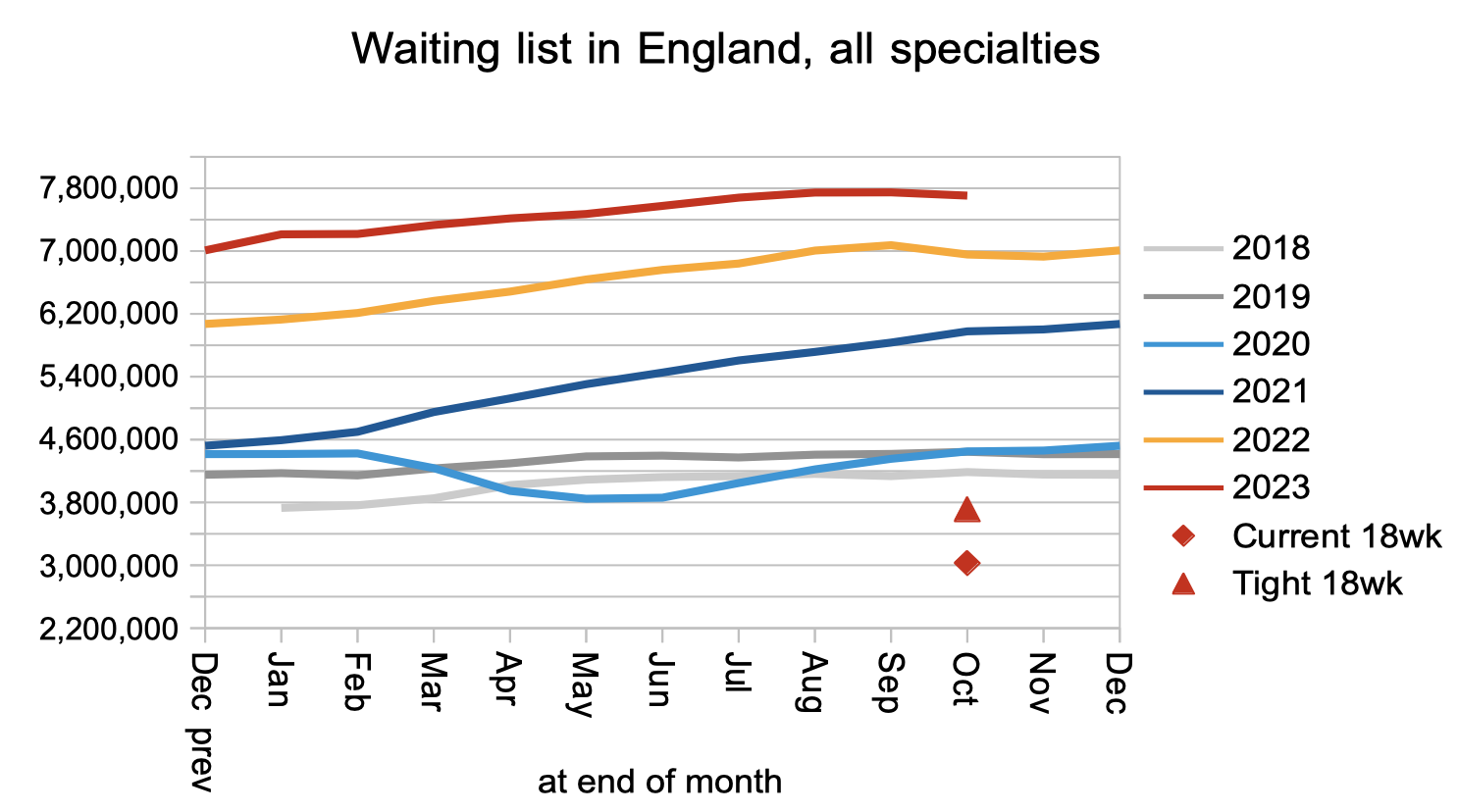
The upshot of all of the above was that the RTT waiting list shrank slightly. It is worth noting at this point that if you tot up the numbers joining and leaving the waiting list, they are not consistent with the change in the size of the waiting list. The discrepancy is bad at national level and gets worse the more closely you look at the detail. It would be helpful (both for local waiting list management and for trust in the statistics) if the quality of the data were improved.
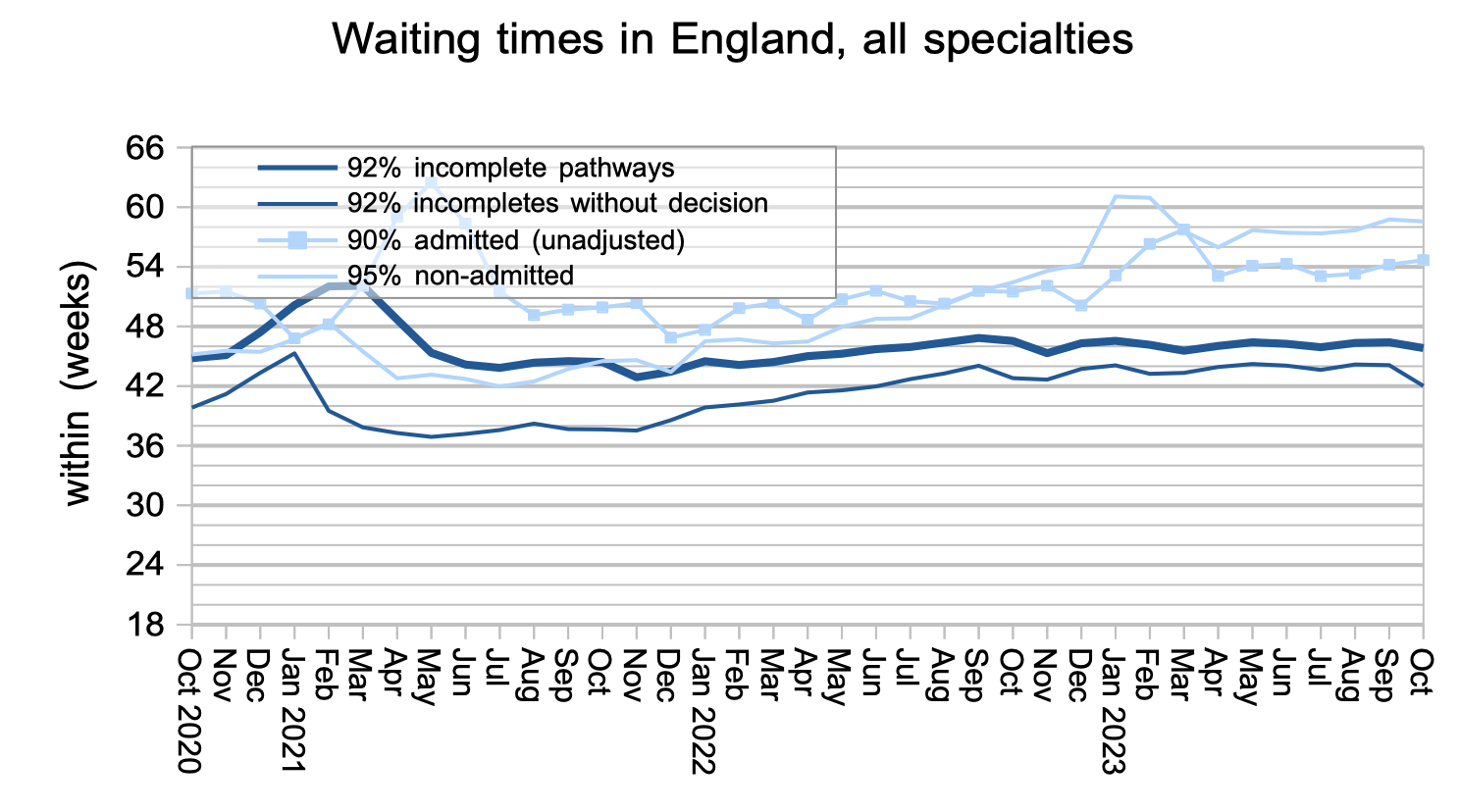
The reductions in waiting list size point to a reduction in waiting times pressures, and waiting times duly fell – slightly for RTT waits, and sharply for the wait to diagnosis and decision. The latter is important because an estimated 27,852 of the patients currently awaiting diagnosis and decision will eventually receive an unexpected diagnosis of cancer, and some others will receive a different urgent diagnosis. The fall to 42 weeks is welcome, but 42 weeks is still far too long to wait for that kind of diagnosis.
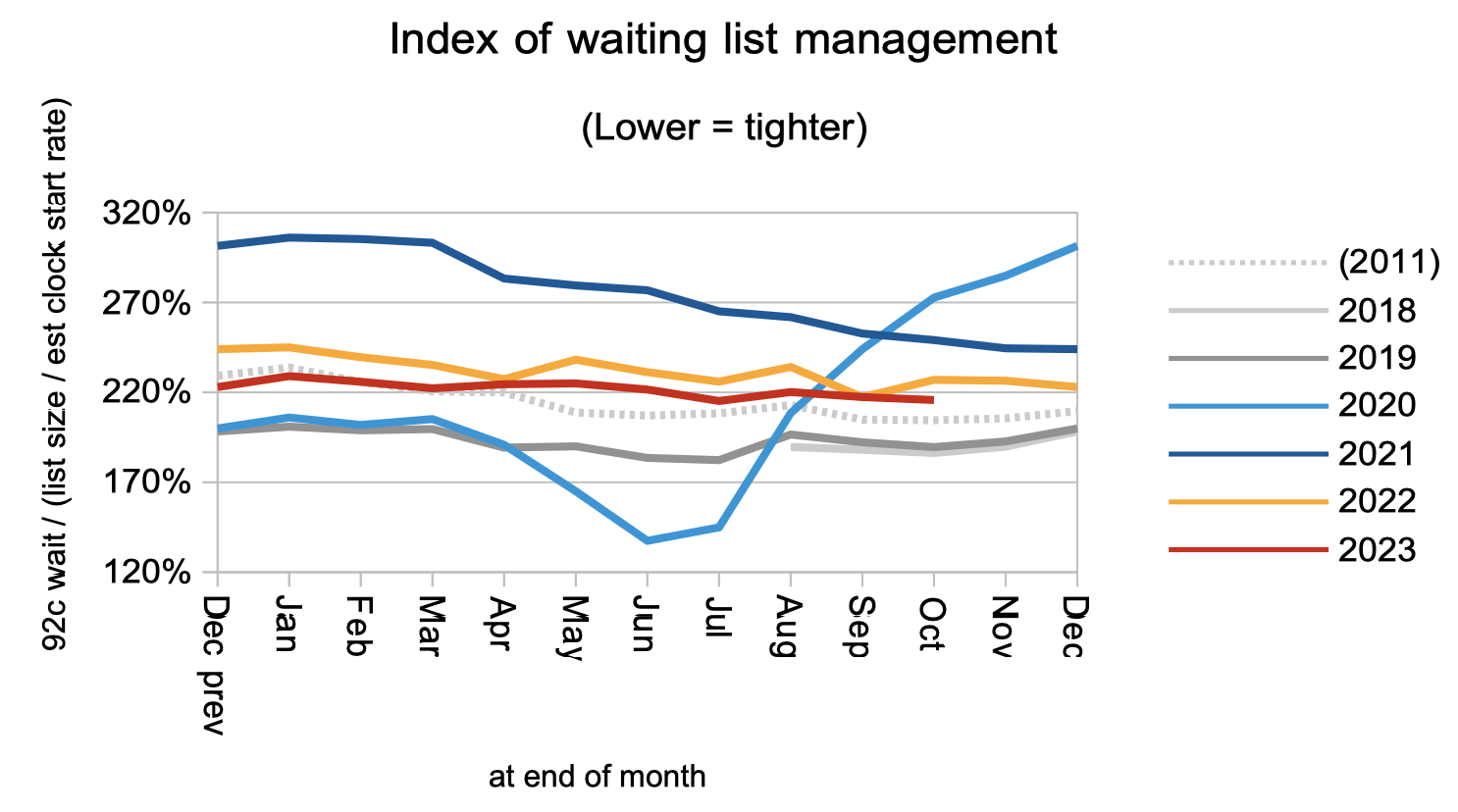
Waiting times are a function of both the size and shape of the waiting list, and the next chart is an indicator of the shape at national level. It remains poor.
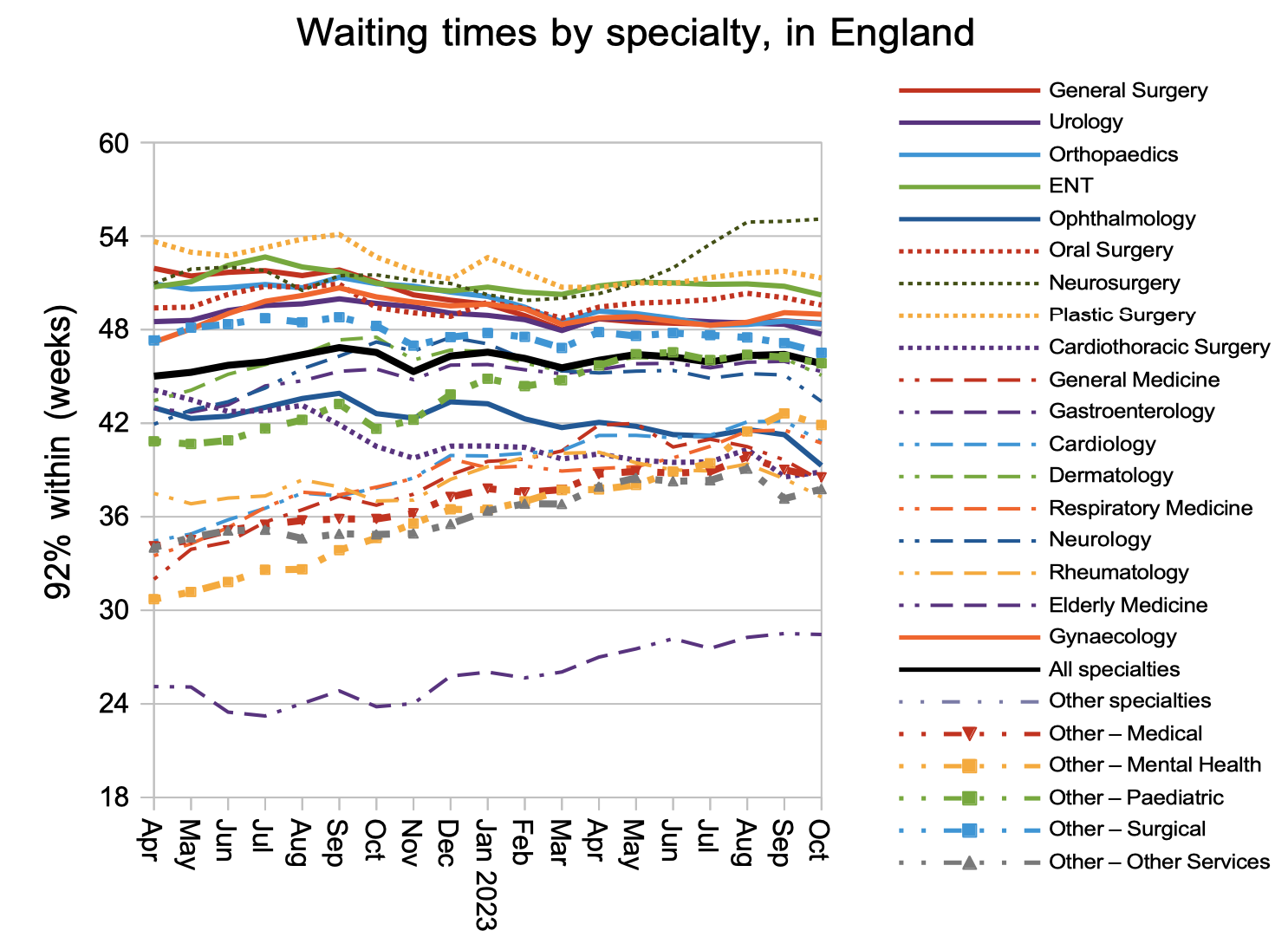
At national specialty level, there was a sharp improvement in Ophthalmology waiting times, which may be attributable to the large increase in independent sector activity in this specialty. Other specialties also improved.
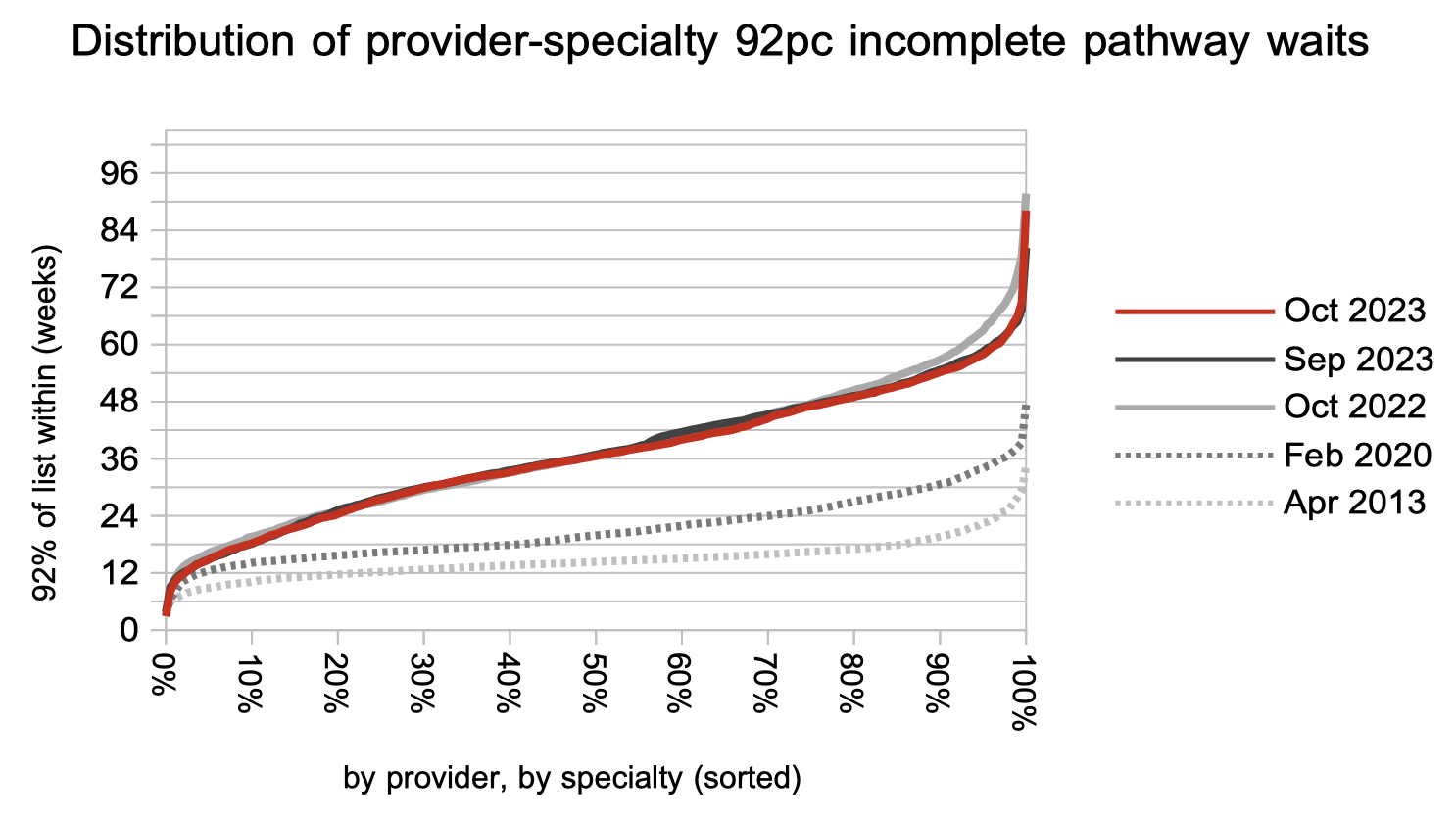
Looking at the full detail by provider and by specialty, we can see that the improvement in RTT waiting times was seen pretty much across the board, with most of the improvement over the last year being at the longer-waiting end of the distribution.
Referral-to-treatment data up to the end of November is due out at 9:30am on Thursday 11th January 2024.