

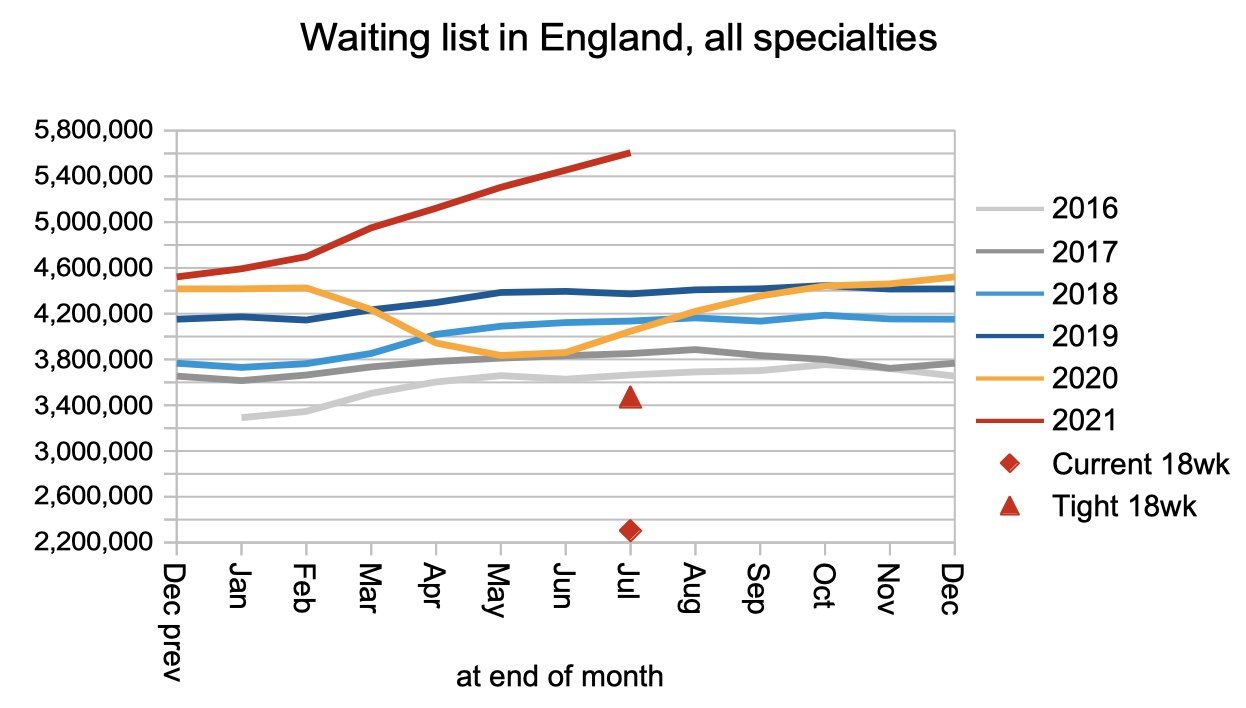
The English referral-to-treatment (RTT) waiting list continued to lengthen rapidly, reaching 5,606,724 patients at the end of July, another record high since the first data was collected in 2007.
The number of ultra long waiters over 104 weeks rose during July from 5,727 to 7,980 patients. Let us not forget that in November 2013 there were only 214 patients waiting longer than 52 weeks.
Waiting times to diagnosis and ‘decision to admit’ rose from 37.2 to 37.6 weeks, meaning that patients with unsuspected cancer are waiting even longer for their cancers to be detected. This matters for patients with other conditions too, because diagnosis means that suitable care can be arranged during the long further wait for treatment.
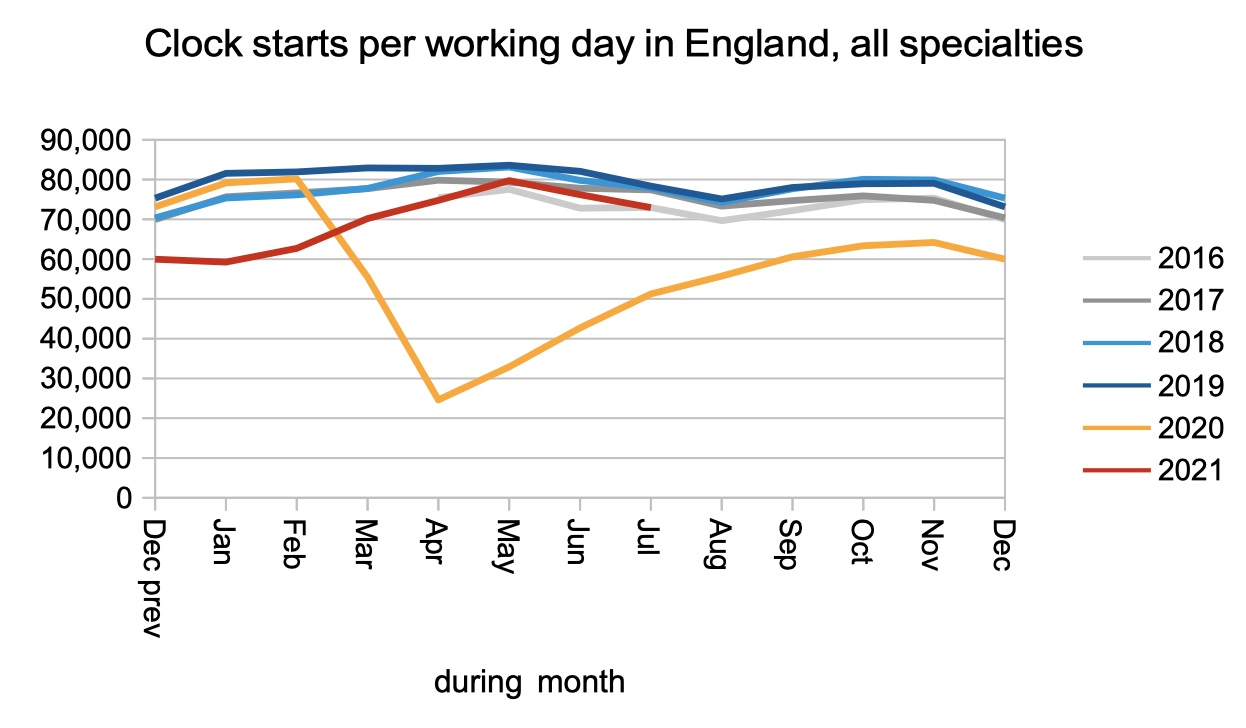
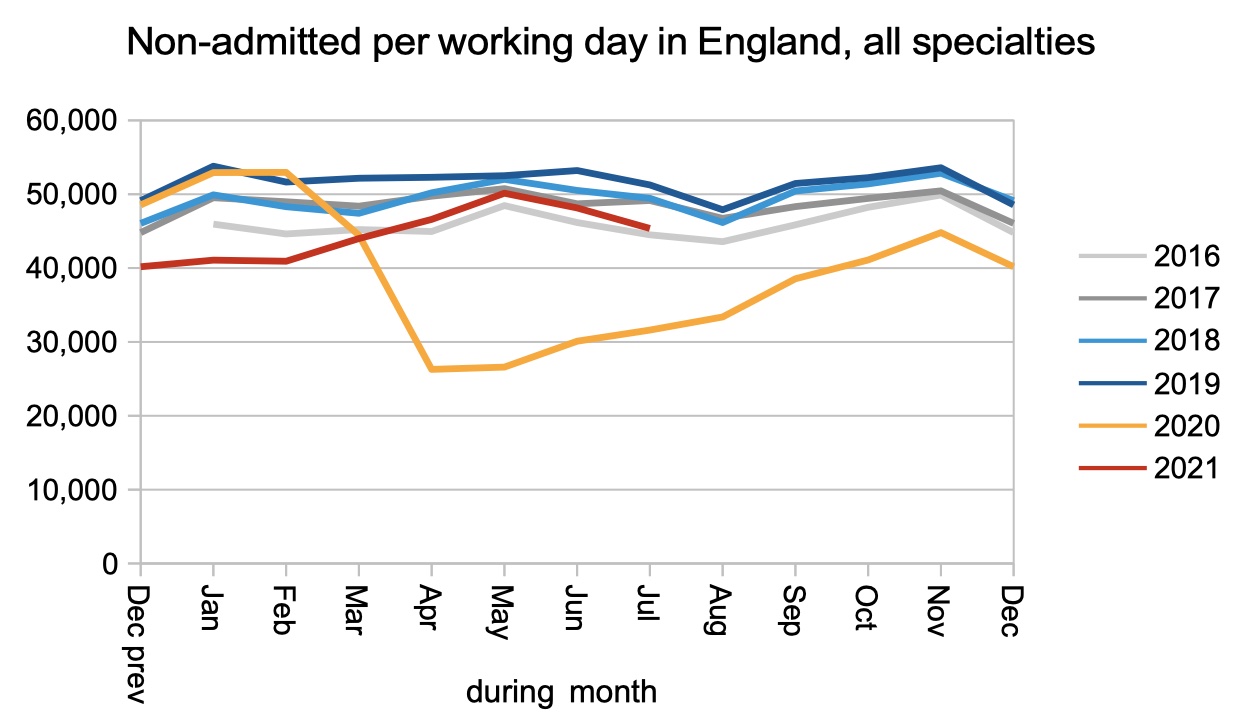
The flow of patients on and off the waiting list has settled into a steady pattern over the summer. New patients are being both referred, and discharged from outpatients or removed, at approaching pre-covid rates. But admissions for inpatient and daycase treatment, which require patients to physically attend hospital and are therefore disrupted by covid infection prevention and control measures, are running somewhat lower than pre-covid rates. The net result is that the waiting list is growing rapidly.
In the following discussion, all figures come from NHS England and NHS Improvement. If you have a national statistic that you’d like to check up on, you can download our waiting times fact checker.
For analysis of waiting times performance at a particular organisation, visit our reports page, or our map of the latest RTT waiting times across England.
The numbers
Since May, patients have been referred onto the RTT waiting list at a similar rate to the pre-covid years. There is no sign yet of the expected surge in demand as ‘missing referrals’ come back, which indicates that patients are continuing to stay away from the NHS for conditions for which they would previously have sought care.
Patients have also been discharged from clinic, or removed from the waiting list for administrative reasons, at a similar rate to the pre-covid years.
However patients are not yet being admitted for inpatient and daycase treatment at a rate approaching the pre-covid years. This sort of care is more difficult to provide because patients must physically come into hospital, and capacity is limited by physical distancing and other covid infection prevention and control measures.
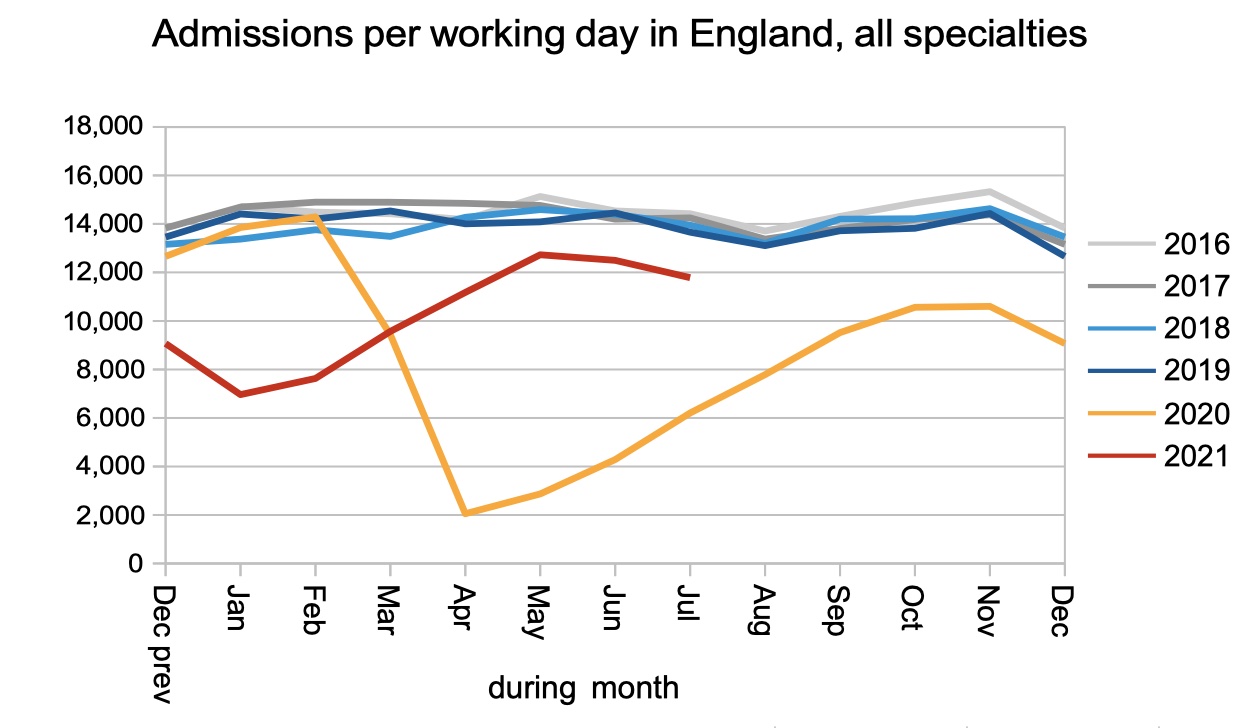
The net result is that patients are being added to the waiting list faster than they come off it, so the waiting list is lengthening rapidly.
A lengthening waiting list is only one driver of longer waiting times, however. The order in which patients are treated matters too, as does the amount of variation in waiting time pressures between one provider and another, and between one specialty and another. There is also some impact from the dramatic fall in referrals during the first covid shutdown, although this effect is now fading.
RTT waiting times are improving at the moment, which is good news. But that is outweighed by the long and worsening waiting times from referral up to decision to admit, which reflect the wait to diagnosis. This is bad news because patients need a diagnosis to detect any unsuspected urgent clinical conditions such as cancer, and so that a suitable management plan can be put in place while they endure the further long wait for actual treatment.

There are huge differences in waiting times between medical specialties, which are largely outpatient based, and surgical specialties, which require patients to attend hospital for treatment.
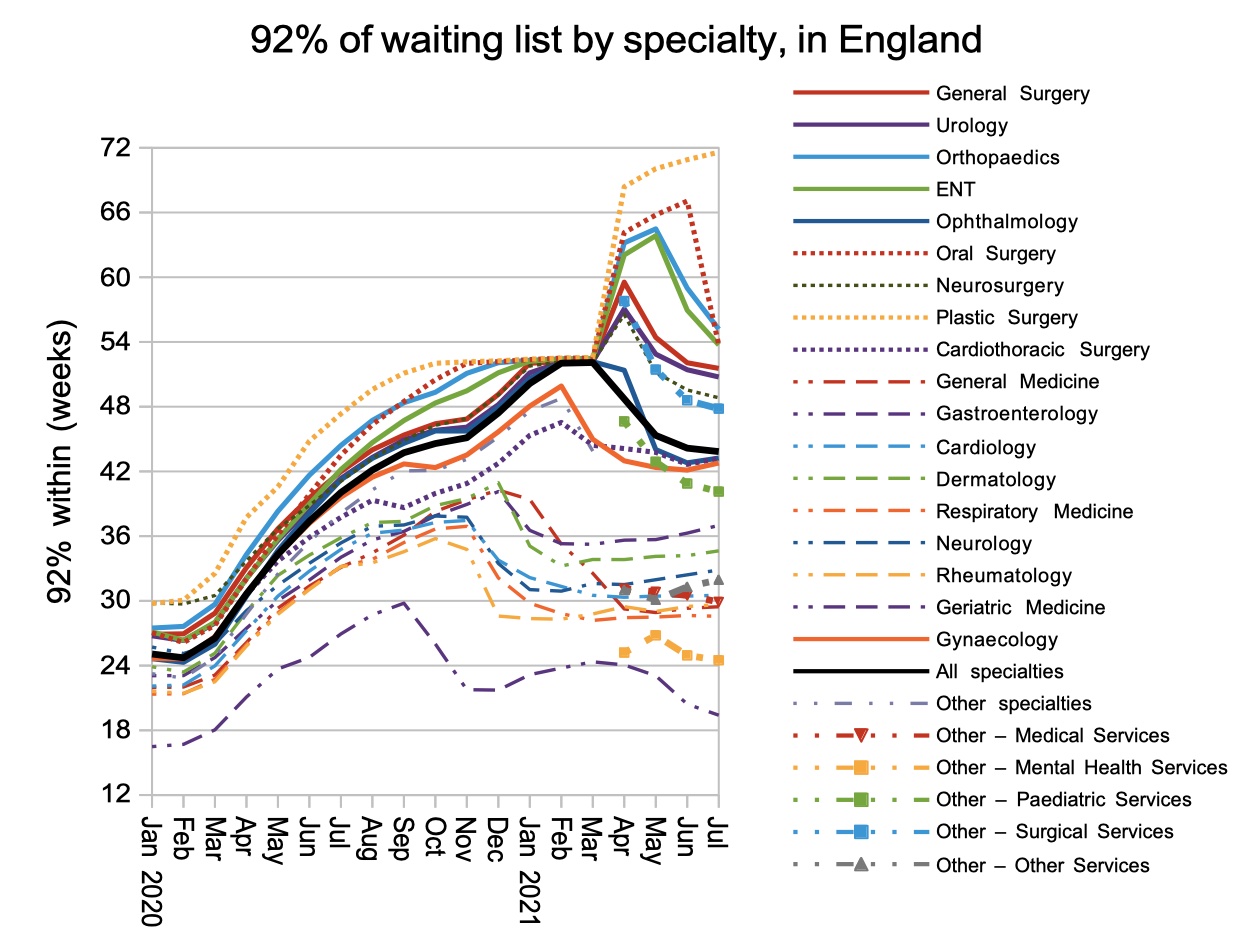
This huge disparity is reflected in the range of waiting times seen across the thousands of local specialties within providers across England. Compare the current distribution with the pre-covid one from Feb 2020, and you can see how unequally covid has hit different services across the country.

Referral-to-treatment data up to the end of August is due out at 9:30am on Thursday 14th October.