

Whenever we model capacity, we have to make some assumptions about performance – things like average length of stay, theatre utilisation, and clinic times. Usually the easiest way is just to measure what happened last year, and assume that will carry on into the future.
That’s how most people start using Gooroo Planner, and it’s nice and easy because Planner can measure past performance for you when you upload your patient-level data. So, by default, your entire model is automatically loaded up with last year’s performance figures.
But sometimes you don’t want to use last year’s performance. You might want to run a scenario with best-quartile benchmark lengths of stay. Or, more realistically, operational managers might say: “I know that last year we only ran ENT daycases at 60% theatre utilisation, but we’ve changed things and next year it will be 80%”.
How can you reflect those expected changes in performance? And how can you make sure that your preferred scenarios are always reflected in the modelling, whether you are running Gooroo Planner for a Board report, for contract negotiations, or for its main function: managing the hospital?
Let me introduce you to the “exceptions table”.
An exceptions table is a kind of statistical dataset; it has all your clinical services down the left, and all your performance assumptions along the top, and the body of the table itself is empty. Well, nearly empty. Every now and again, there’s a number: like 0.8 (80%) under theatre utilisation for ENT daycases. Like this example:
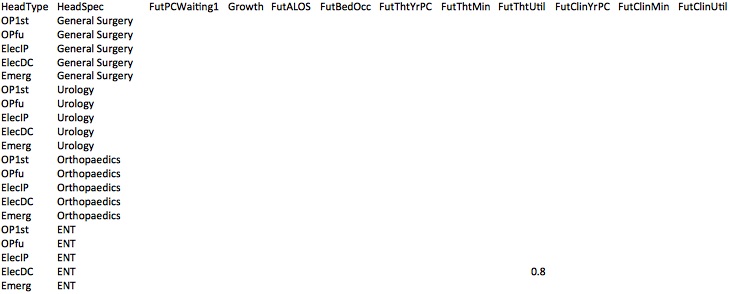
When you upload data into Gooroo Planner (either on-screen or automatically) this is the last file to be uploaded. Whenever there is already a number in the exceptions table, you can ask Gooroo Planner to overwrite it with this one.
![]()
The exceptions table might sound like a minor bit of process, but it has huge organisational implications. When the exceptions table’s purpose is explained to operational managers and clinicians, the mood immediately flips from “what is this doing to us?” to “you mean, I’m in control of this?”, because they are essentially being handed control of every performance assumption, in every scenario, in every planning model.
And not just performance assumptions – the exceptions table can also include how activity will be profiled week by week into the future, and even how you think demand varies seasonally in a typical year.
A powerful tool like this needs to be in safe hands. Whoever curates this intelligence will probably find themselves taking a pivotal role within the organisation, and having corporate responsibility for making sure that capacity planning is understood and agreed by operational managers.
To perform this important function, this individual (let’s call them “Gooroo liaison”) will need to understand the Gooroo Planner modelling in detail, so that they can:
- interpret the results to operational managers, so that they understand its implications, and are able to say when they think any performance assumptions, or the way that pathways are reflected, need to be changed;
- change the performance assumptions in the exceptions table, and make sure the current version is always included in any new models;
- explain more complex changes to the information analysts (who maintain the database queries that feed Gooroo Planner), in language that they can understand and reflect in their query code.
If that sounds like a lot, remember what we are achieving here. Perhaps for the first time, operational managers will be kept up to date with, understand, and have ongoing control over the corporate capacity planning model… which means they are much more likely to take action when the modelling says they should.
By contrast, think of all the contracting models and annual capacity plans that have been drawn up and painfully negotiated in the past. How many of those were ever implemented in real life?
There is an opportunity here to bring regular, detailed planning to life in the NHS. The innocuous-sounding “exceptions table”, and the key individual responsible for Gooroo liaison, are right at the heart of it.